This 18-year-old female presents with a palpable soft tissue mass subjacent to the first metatarsophalangeal (MP) joint that she has noticed for 1-2 months. It is painful with shoes and ambulation, and you are evaluating her for a soft tissue tumor. What is the cause of her problem, and what pertinent negatives must you notice?
 Axial T2
Axial T2
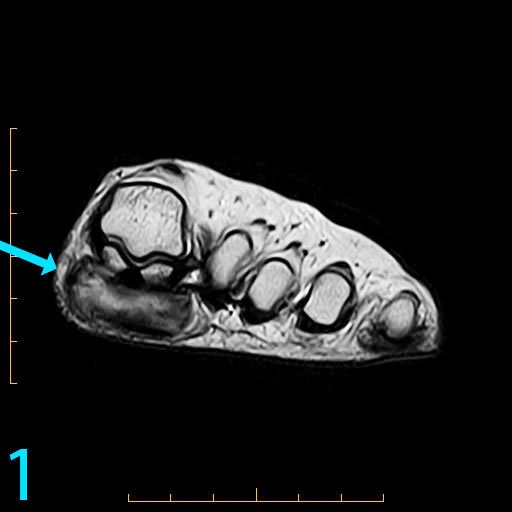
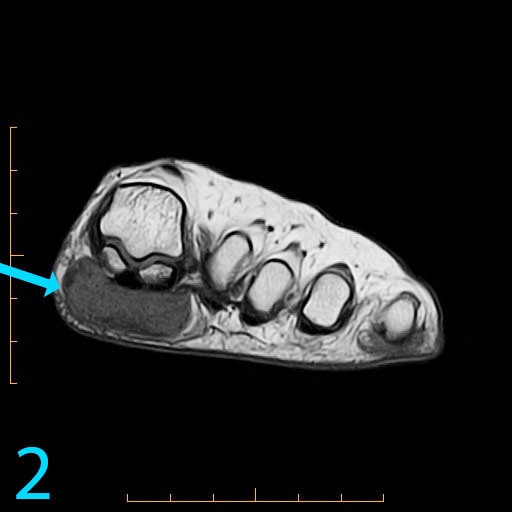 Axial T1
Axial T1
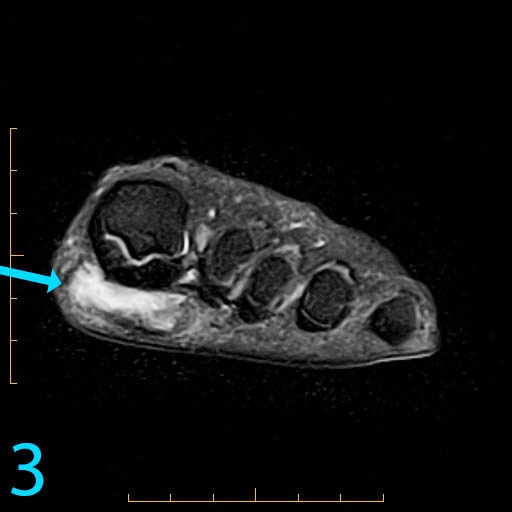 Axial PD fat-sat
Axial PD fat-sat
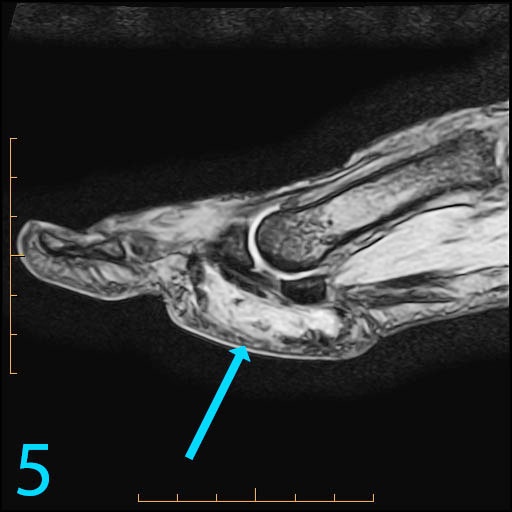
 Sagittal T1
Sagittal T1
 Sagittal GRE
Sagittal GRE
 Coronal T2
Coronal T2
This patient has a so-called "pressure lesion" due to ambulation, with associated adventitial bursa/pseudobursa formation within. It is a chronic process. This is manifested as a large, ovoid mass-like structure within the subcutaneous soft tissues along the plantar aspect of the first MP joint and sesamoid bones (arrow). It is well-circumscribed and demonstrates a mildly lobulated configuration. There is peripheral signal hypointensity indicating a rim or rind of fibrosis, and there is intermediate to high T2 signal centrally, suggesting a component of complex fluid. The major differential diagnosis is fibroma of tendon sheath. This is a counterintuitive diagnosis as fibrous lesions are typically dark on all pulsing sequences. But, fluid signal from the tendon sheath may be found in this specific fibrous tumor. So, fibromas of tendon sheath are typically hyperintense centrally.
While the lobulation of the lesion medially is reminiscent of plantar fibromatosis, the constellation of findings remains most compatible with a giant pressure lesion. Fibromatosis (non-aggressive type) occurs more proximally in the middle aponeurotic cord of the plantar fascia. The findings are not suspicious of an aggressive neoplastic lesion (based on location and concentric shape), and you can also rule out MP joint capsulitis and Morton's neuroma because of location. You should always rule out plantar plate tear along the second MP joint on thin section sagittals if you have a large pressure lesion under the second metatarsal head. For more case review, visit MRI Online.
[gravityform id="4" title="true" description="true"]